
HIV and Aging
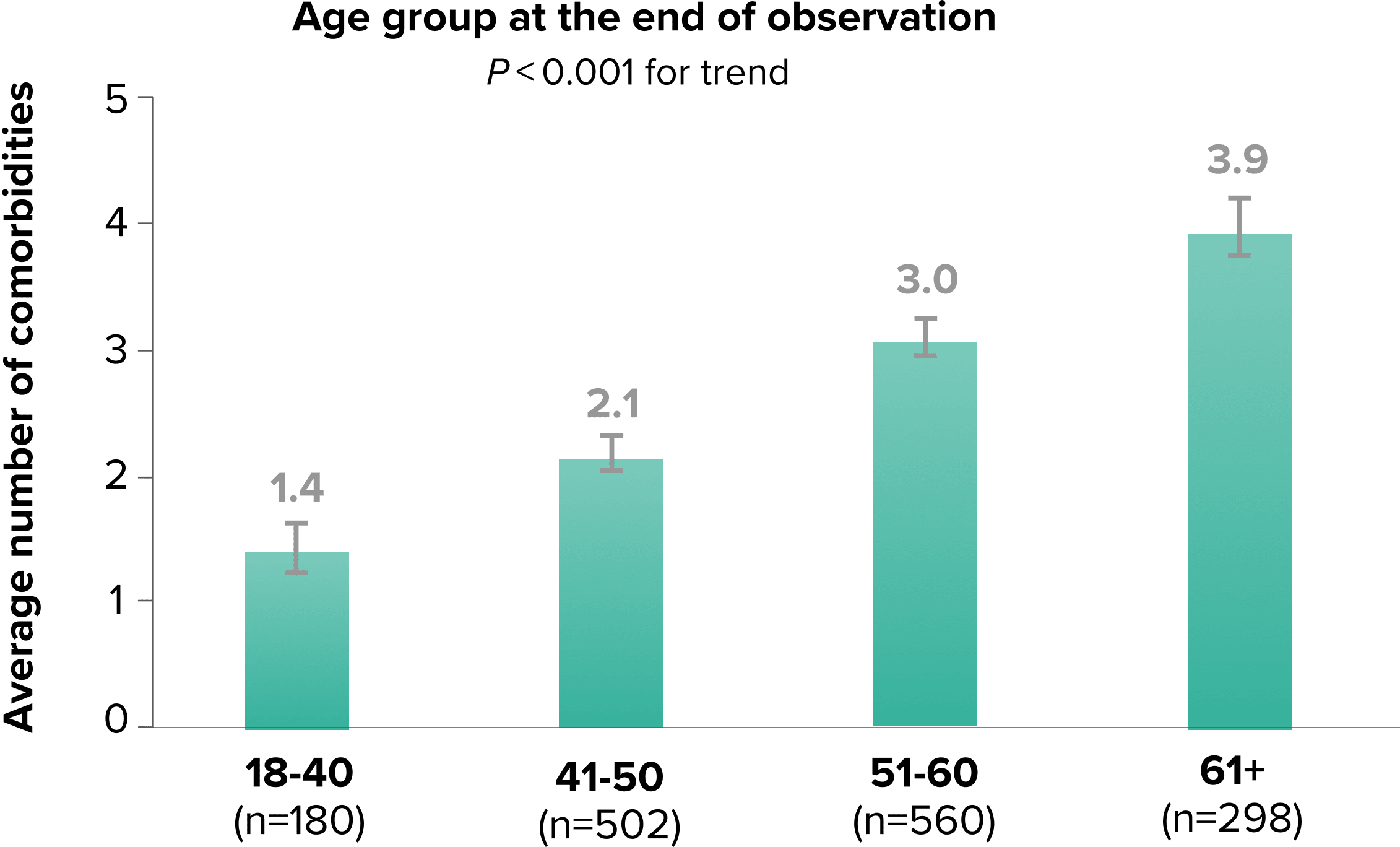
The HIV Population Is Aging1-3
According to the CDC, in 2021, more than 53% of PWH were ≥50 years of age4
How do you identify barriers that may affect your patients’ treatment goals?
Explore some of the key factors that Dr. Joel Gallant and Dr. Calvin Cohen considered to achieve durable viral suppression.